IRAQ’S HEALTH SYSTEM AT RISK: THE STRUGGLE TO FIGHT COVID-19 AND SAVE LIVES
The COVID-19 pandemic, which for the first few months seemed to mysteriously spare Iraq’s exposed population, is now hitting the country of 39 million and its under-resourced health system hard. The main cause has been poor compliance with social distancing policies by many Iraqis who haven’t taken the pandemic seriously or prefer to risk disease rather than suffer the economic costs of extended lock-down. Meanwhile, poor policies and poor conditions at hospitals are causing many of them to spread the virus rather than prevent new cases.
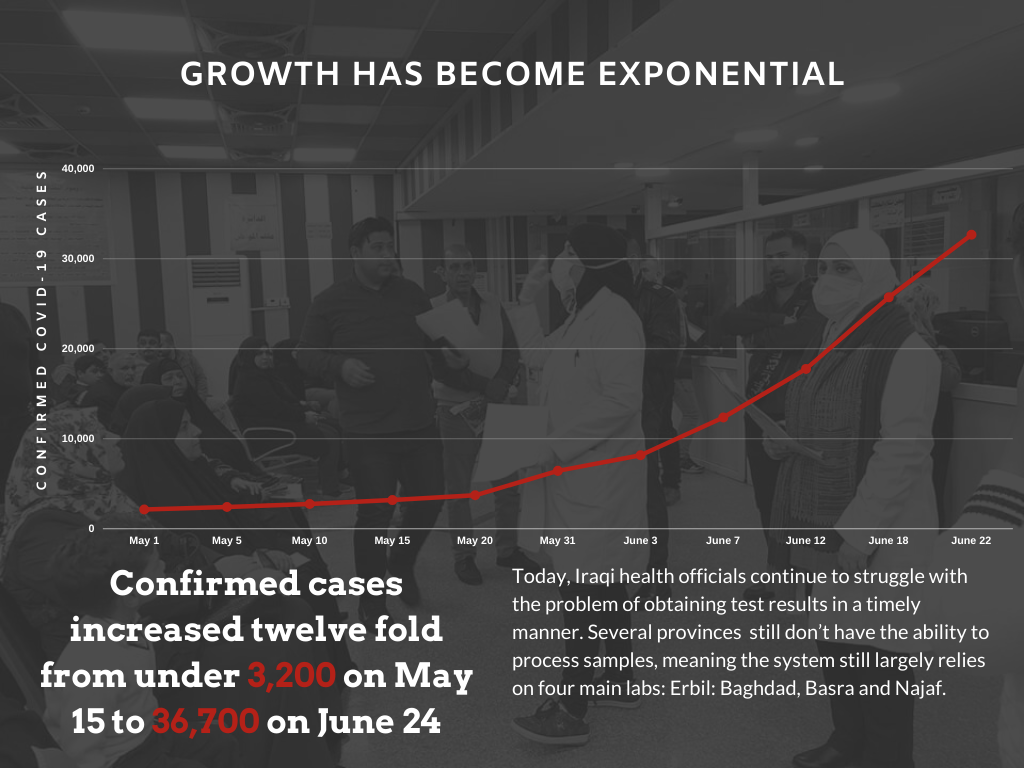
Case growth has become exponential since mid-May. The second half of May coincided with the end of Ramadan and the Eid al-Fitr holiday—major social occasions during which Iraqis are accustomed to shopping, attending large gatherings at mosques and concert halls, and visiting friends and relatives. As early as June 1, the World Health Organization (WHO) warned that there were “widespread anecdotal reports of crowded public spaces across Iraq—including markets and shopping malls.” Iraq’s Health Minister pleaded with Iraqis to take the outbreak seriously and stay home due to the “critical situation” in the country. The director of Iraq’s Ministry of Health in Baghdad voiced concern that poor compliance with preventive measures threatened to overwhelm the national health care system and exceed its hospital bed capacity. During this period, confirmed cases increased twelve fold, from just under 3,200 on May 15 to 36,700 on June 24. Among the latest victims of the outbreak was Ahmed Radhi, Iraq’s beloved soccer legend who was a pillar of Iraq’s national team and famously scored the country’s only World Cup goal in the 1986 FIFA World Cup in Mexico. Simple data analysis of the figures released by the Ministry shows accelerating spread of the disease. The sharpest increase occurred from June 3-5, when Iraq saw the largest daily jumps, exactly two weeks after the Eid holiday. That rapid increase in new cases prompted Iraq’s top cleric, Ayatollah Ali al-Sistani to urge Iraqis to observe social distancing and comply with the instructions of health authorities. In his message, Sistani reminded Iraqis that the country’s weak health care system can’t provide enough care for the “increasing numbers of patients who have overwhelmed the hospitals.”

The situation at many of Iraq’s hospitals deteriorated rapidly, as waves of new cases exposed their capacity to cope with extraordinary pressure and overwhelmed their overworked and under-resourced staff. Dr. Jafar Alaa, Head of Programs at the Iraq Health Access Organization (IHAO), said this of the difficult times facing Iraq’s health workers: “When you talk to health staff you can sense their frustration and the bleak view of the situation… There is so much stress. Many of their colleagues caught the virus and the numbers of cases and deaths keep rising and they are not able to do much about it.”
Testing capacity improves, but delays abound. Iraq managed to quadruple its testing capacity over the last six weeks, from about 3,000 to over 12,000 samples per day. That more testing leads to more confirmed cases is to be expected. But the worrisome trend is that the ratio of positive cases to tested samples is accelerating rapidly: from 0.6% on April 16 to 2.1% on May 16 to 14.5% on June 19. During the first 22 days of June, confirmed cases increased by an average of 7.73% daily. At this rate, more than 2.8 million Iraqis could be infected within the next 60 days.
A new spike is expected to occur next week, when Iraq ramps up testing from nearly 13,000 samples per day now to 20,000 per day. But the number of confirmed cases may appear to plateau around 1,800 new cases per day as a function of limited testing capacity rather than slower transmission.
Testing accuracy and reliability had obscured the extent of Coronavirus spread during early stages of the outbreak. According to Dr. Ghassan Aziz, an Iraqi epidemiologist with whom we spoke, many patients whose symptoms made doctors believe they had contracted COVID-19 tested negative, due to a number of factors that impacted accuracy:
- Quality of testing kits
- The limited number of sample processing labs meant that most samples had to be processed at the central public health laboratory in Baghdad. Many samples were destroyed by heat, given the difficulty of maintaining cold chain transportation in Iraq’s warm weather.
- Problems with preparation for sample transportation, including virus transport mediums, meant that entire batches tested negative.
- Many staff tasked with taking samples with swabs lacked the knowledge or training to do so properly. In many cases staff took nasal swabs instead of proper nasopharyngeal samples because patients didn’t cooperate or staff stopped short when they sensed the patient might sneeze.
The virus is taking its toll on health workers. Escalating COVID-19 conditions in Iraq is particularly alarming because the virus is spreading rapidly and at high rates among doctors, nurses and other health workers, threatening to deplete the health care system’s most irreplaceable assets. WHO data for COVID-19 in Iraq show that of the 25,717 total cases reported on June 19, 1,720 were health care providers; health care providers represented 6.6% of total cases and 8.4% of active cases. In the U.S. there were 80,249 cases of COVID-19 among health care workers out of 2,155,572 total cases on June 18, representing 3.7% of total cases, according to CDC data. This could spell disaster for Iraq; while Iraqi health care workers are twice as likely to contract COVID-19 than the general population, Iraq has far fewer doctors and other health workers than many countries. The U.S. has almost four times as many doctors per 1,000 people, according to World Bank data. Dr Aziz warns that many hospitals could fall apart within one to two months because of rising infections among staff.

The financial crisis is gutting the health care system. The acute impact of recent decline in Iraq’s oil revenue is compounding the effect of chronic under-investment in the health sector. Sulaymaniyah, a province that appeared to be on the verge of beating COVID-19 in May, is now registering some of the highest levels of new cases in Iraq. The relapse appears connected to the decision on June 2 to discontinue the curfew and reopen the economy, this after a government announcement to extend the curfew caused public uproar in Iraq’s Kurdistan region. In addition, the regional government’s inability to pay salaries for months prompted doctors and other health staff to go on strike. The provincial director of health warned that hospitals and health centers could stop functioning altogether.
Social impact. Fear, isolation, economic distress and a sense of helplessness are some of the by-products of the pandemic taking a toll on society and giving rise to growing mental health challenges. A recent survey of internally displaced and returnee communities in various provinces by the UN NGO protection cluster indicated that “nearly three quarters of respondents reported that protection issues have significantly increased since the beginning of the COVID-19 crisis.” The study explains that respondents pointed to “increased feelings of trauma, stress and anxiety” as the main complaints and that “women, girls, children, people with disabilities and the elderly” were experiencing “poorer mental health and psychosocial well-being.” Another organizational study found that reports of gender-based violence increased by 65% since the pandemic started. Of those cases, 94% represented “domestic violence perpetrated by a household member.” Most respondents attributed this spike in domestic violence to isolation.
Health administrators prioritize staying open, ignoring risk. Doctors in various hospitals have been complaining that hospital administrators are ignoring the need to isolate medical staff who have been in contact with colleagues or patients who have tested positive for COVID-19. Instead these doctors, often young interns, say administrators are forcing them to keep working, raising the risk of transmission among staff, patients and visitors, raising concern that some medical staff are unintentionally becoming mass spreaders. As one doctor pointed out to EPIC, hospital managers are reluctant to test staff because if doctors and nurses test positive they would have to let them go home, increasing the workload for the remainder of an over-worked staff. Some doctors’ have suggested on social media that managers’ motivations might be more self-serving. At al-Habibiyah hospital in Baghdad’s Sadr City, the hardest hit district in Iraq, the director rejected suggestions to isolate staff that came in contact with two nurses who had tested positive. The director stated, “no way I’m closing a hospital in Sadr City,” indicating to observers his desire to look good in the eyes of his superiors and other powerful local figures. Interns at al-Hay Hospital in Wasit Province told a similar story on social media. After three interns tested positive, hospital managers forced seven others who shared dormitories to keep working with patients, even when some of them began to show symptoms typical of COVID-19.
Death statistics are not revealing the full picture. While Iraq’s health authorities are transparently reporting deaths from COVID-19 on a daily basis, these numbers do not account for deaths outside of hospitals. Although doctors who write death certificates for those who die at home report increasing numbers, there are no officially published statistics for proper analysis. Anecdotal reports from these doctors are nonetheless alarming. A doctor at a hospital in Sadr City recently wrote on social media that about six weeks earlier he had issued four death certificates for people who died at home during one 72 hour period, but that his colleagues are now issuing up to 25 death certificates each day. Comments by doctors from other hospitals suggest a similar trend. Hospitals in Baghdad are issuing three times as many death certificates for deaths at home as they did in April. According to Dr. Aziz, hospitals continue to follow pre-pandemic practices of issuing most death certificates without autopsy. Deaths at home of people over 55 with common chronic conditions such as diabetes, hypertension, heart disease and brain strokes are automatically attributed to complications of these conditions.
Test results still face delays. Although Iraq has significantly expanded testing capacity (from approximately 1,500 samples/day in early April to approximately 12,000 samples/day), Iraqi health officials still struggle to obtain test results in a timely manner. Several provinces, including Dhi-Qar, which recently received sample processing devices, still have no capacity to process samples. The Iraqi health care system still largely relies on four main labs in: Erbil, Baghdad, Basra and Najaf. Patients, and even doctors, sometimes wait a full week before they receive test results. Delays often mean infected people are left to move about freely, or that recovered people are held in isolation longer than necessary, occupying hospital beds that more acute cases desperately need.
Misguided testing policies waste precious resources. Iraqi health authorities put a lot of emphasis on field testing as a form of active surveillance for the virus (which the Ministry of Health labels as random even though it is not). Dr. Aziz criticized this strategy as a misuse of limited resources, arguing that it wastes valuable staff time, effort and resources, while exposing health workers to unnecessary risk, putting them in contact with large numbers of people outside hospitals. As currently practiced, a field test is initiated after a person tests positive. The local primary healthcare center selects targets for testing from among the person’s neighbors with whom s/he was in close proximity. If staff suspect that one or more neighbors have contracted the virus, they run a rapid antibody test. If positive, the staff then run a PCR test. A problem with this plan is that a positive rapid antibody test indicates that a person is either recovering or fully recovered already; results therefore have little or no use in detecting new infections early enough for effective treatment or prevention from further spreading. Delays in obtaining test results can give the false impression that people are healthy when in fact they aren’t.

Non-life-saving visits continue. Hospitals and clinics in countries impacted by COVID-19 around the world have halted the provision of any services but emergencies to free up resources to deal with COVID-19 and avoid unnecessary human contact that increases the risk of transmission to staff and patients alike. This has not been the case in Iraq, where each clinic and hospital continues to serve hundreds of patients each day for non-life-threatening conditions at departments from dermatology to dentistry to nutrition. This policy causes damage in two ways by contributing to transmission through countless incidents of unnecessary contact, and by diverting staff time and resources away from effectively managing the pandemic. Liberal admission policies for mild cases of COVID-19 have also contributed to pressure on hospitals, using thousands of hospital beds during the early stages of the outbreak, and ignoring the possibility of cases reaching levels threatening to exceed the system’s capacity. As the WHO representative for Iraq pointed out in a recent interview with Iraq Oil Report, authorities have been hospitalizing all confirmed cases, even mild ones who would be told to stay at home in many other countries.
The Health Ministry’s belated attention to this problem resulted in a policy announcement on June 19 that the Ministry will free up a number of hospitals to exclusively treat COVID-19 patients, and repurpose public buildings to add about 2,400 beds for the city of 8 million. Non-government entities, such as charities associated with the shrines of Najaf and Karbala, are launching their own initiatives to quickly assemble several field hospitals, each with 60-80 beds for COVID-19 patients, in a half dozen provinces. Although these improvised field hospitals are being equipped with large numbers of beds and equipment, the real challenge is finding enough staff to run them. The Director of the Karkh Department of Health, overseeing Baghdad’s western half, has urged health professionals, including dentists and pharmacists, to volunteer to serve patients in one of the field hospitals upon its opening, but it seems unlikely there will be enough health professionals to fill the gaps.
Health authorities are also attempting to divert some cases away from hospitals. New directives will divert suspected cases to local health clinics to reduce pressure on hospitals and the Public Health Department within Iraq’s Ministry of Health sent out guidelines in early June with indicators for treatment at home and indicators for admission. The department decided that, going forward, only people with severe symptoms will be admitted. The goal is to limit admissions while asking those with mild and moderate cases to stay home where they would be visited by doctors from the nearest health center. However, stable patients with mild COVID-19 symptoms are still entering isolation wards that should be reserved for patients in critical condition.
Against this bleak backdrop, the situation may look desperate, and it is indeed extremely challenging. But there are still measures available to prevent the worst. Based on our observations and analysis of conditions, and our discussions with epidemiologists and public health experts, EPIC has developed the following recommendations on measures to mitigate the next phase of the COVID-19 crisis in Iraq.
Recommendations:
- Halt visits to clinics and hospitals for non-urgent services. Consider establishing a system for tele-medicine for health consultations other than COVID-19 to provide medical advice to those who need it, thereby eliminating or at least reducing visits for non-life-threatening conditions.
- Consider taking decisions on curfews and movement restrictions at the district level, instead of national or provincial levels. It is no longer feasible to do contact tracing everywhere. Iraq needs to adapt its response for each region, depending on the level of spread among other factors. For low incidence districts, seal them off, and conduct contact tracing and isolation/treatment. For districts with high incidence, do more to stop transmission within.
- Work to control secondary infections at health facilities, such as those occurring when COVID or non-COVID patients or their accompanying relatives contract the virus or transmit it to a staff member with whom they come in contact. This requires stronger infection prevention control (IPC) measures, including: stronger IPC protocols at hospitals and health care centers; quality personal protective equipment (PPE) available to doctors, other health workers, and first responders, as well as families caring for relatives with COVID-19; and training on the proper use of PPE and how to prevent secondary transmissions.
- Give all medical staff, including those with non-respiratory specialization, the training they need to diagnose and manage COVID-19 cases.
- Recognize the critical role played by support staff at hospitals who work long hours in high risk environments for little compensation (as little as 4-6 USD/day) and explore ways to address their needs.
- Expand testing for all health workers and support staff, and establish a system for shift work in which staff works for a week, then isolates for two weeks, to better identify and isolate staff members who have contracted the virus.
- Establish an emergency program to secure and deliver essential life-saving supplies, such as oxygen, of which many Iraqi hospitals, especially in Baghdad, report shortages.
- The Iraqi government and KRG should establish hotlines staffed by health professionals to field inquiries, and should make use of tele-medicine to remotely help mildly symptomatic patients at home, especially for routine consultations. WHO has established a protocol for home care that should be widely encouraged and used, especially given the risk of secondary infections at health care facilities.
- While fighting COVID-19, far more will be needed to offset the harm done to day laborers and others who depend on their work to feed their families. This has been one of the main causes of curfew and social distancing violations. Related measures should include the delivery of food baskets and hygiene kits to under-resourced families with COVID-19 who have self-quarantined to protect their communities, and mobilizing resources for those most financially impacted by the economic downturn, lock-downs, and higher prices. During lock-downs, case-by-case exceptions should be made for essential workers and day laborers, provided they are screened and cleared for work, and provided they work outdoors, or in ventilated areas, use proper social distancing, wear masks, and take other preventive measures.
- Issue new guidelines and legal protections for hospitals to cease issuing death certificates for those who die at home without autopsy.
- Continue to step up efforts to normalize social distancing behavior Iraqi in society, and to fight rumors and conspiracy theories about the virus. Establish strict measures to prevent crowding at government offices and other public buildings providing essential services (such as banks), where anecdotal reports have shown repeated incidents of unsafe distancing.
- The pandemic is stressful. It causes fear and anxiety, and countermeasures lead to feelings of isolation and other serious problems. Iraq is seeing a significant increase in mental health needs, domestic violence, and gender-based violence (GBV). Iraq and the international community must do more to support interventions to counter the pandemic’s social impact in Iraq.
Iraq’s health system is facing an extraordinarily acute challenge. Medical staff are overstretched and under extreme stress. Hospitals are woefully under-resourced and overrun with symptomatic patients. Trainings on IPC protocols, including the proper use of PPE, and COVID-19 treatment guidelines are scarcely available. This situation is simply unacceptable. The U.S. and international community must work swiftly with the Iraqi government to direct resources to where they are needed most. And right now, far more is urgently needed to shore up Iraq’s increasingly hard hit health system before it is completely overwhelmed.